Find Treatment By
Rehabs by Location






Learn
About Us
Recovery.com combines independent research with expert guidance on addiction and mental health treatment. Our mission is to help everyone find the best path to recovery through the most comprehensive, helpful network of treatment providers worldwide.
Advisory Council
Our advisory council brings together leaders in behavioral health, technology, and business. Their diverse expertise ensures our resources and product are innovative, evidence-based, and effective. They guide our mission as accomplished individuals dedicated to improving the landscape of addiction recovery and mental wellness.
The Best Behavioral Health Admissions Process: 7 Must Answer Questions

Table of Contents
- 1. Do You Have A Documented Call Flow?
- 2. What Is Your True Answer Rate?
- 3. What Happens When You Miss a Call?
- 4. Do You Score Your Calls?
- 5. How Fast Do You Respond To Form Submissions & VOBs?
- 6. Do You Have A Living “Obstacle Overcomes” Document?
- 7. Do You Role Play With Your Admissions Team?
- The Bigger Question
Marketing generates inquiries.
Admissions determines whether those inquiries turn into placements.
Many behavioral health centers focus intensely on driving more calls, more form fills, and more traffic. Far fewer take a hard look at the system that handles those inquiries once they arrive.
If census fluctuates or conversion feels inconsistent, the issue is often not lead volume.
It is the admissions infrastructure.
Below are seven questions every behavioral health center should be asking about its admissions process.
1. Do You Have A Documented Call Flow?
If you asked each admissions coordinator on your team to explain your program, would their answers sound aligned?
Or would they be dramatically different?
If every rep tells the story of your center differently, gathers information in a different order, or transitions to next steps inconsistently, you do not have a standardized admissions process. You have individual communication styles.
A call flow exists to create consistency.
It standardizes how your program is explained.It standardizes how information is gathered.It standardizes how conversations move toward action.
Most importantly, it standardizes the caller’s experience.
When grounded in Motivational Interviewing principles, a strong call flow uses open-ended questions, reflective listening, affirmation, and autonomy support to guide rather than pressure.
But structure matters just as much as empathy.
A disciplined call flow takes control early in the opening of the call. It gathers key qualifiers such as age, primary concern, location, and insurance before going deep. It sets expectations about assessing fit before discovery begins.
That order protects everyone’s time.
If someone is not clinically appropriate or financially viable, they should not have to recount their entire life story before learning that. Asking qualification questions early honors dignity and efficiency.
Once basic fit is established, the conversation moves into deeper discovery, exploring impact on work, relationships, and personal wellbeing. The admissions coordinator clarifies recovery goals and reflects both pain and desired outcomes back to the caller to ensure alignment.
Only after that alignment does the coordinator ask permission to explain the program and position it through a biopsychosocial model that connects biological, psychological, and social care to the caller’s specific needs.
The close is not a hard sell. It is a confident move to the next clinical step, such as insurance verification or a confidential pre-screen.
When implemented correctly, a call flow does more than improve conversion.
It ensures every caller feels heard.It ensures every rep represents the center consistently. It respects time.It creates the most likely outcome that someone takes a meaningful step toward treatment.
If your team cannot articulate the same structured path from open to close, that is the first system to tighten.
If you would like a starting point, we have published an example behavioral health call flow template that centers can adapt for their own admissions teams.
2. What Is Your True Answer Rate?

High-performing healthcare and behavioral health call centers typically strive for an answer rate of 90 to 95 percent or higher during business hours. World-class teams often operate at 95 percent or above.
If your answer rate is below 85 percent, there is likely meaningful revenue leakage. Below 80 percent, missed calls are almost certainly impacting census.
Before improving it, you need to calculate it clearly.
Answer Rate = (Total Calls Answered Live ÷ Total Inbound Calls) x 100
For example, if your center receives 250 inbound calls in a week and answers 200 of them live, your answer rate is:
(200 ÷ 250) x 100 = 80 percent
That means 20 percent of callers never reached a live person.
Now ask yourself whether 1 out of every 5 people reaching out for help should be going to voicemail.
How many inbound calls are actually answered live?
How often do callers reach voicemail? What happens after business hours?
People seeking treatment often call multiple centers within a short window. The first center to answer and build trust frequently earns the admission.
Answer rate is not just an operational metric. It is a revenue metric.
If calls are consistently missed, conversion will suffer regardless of marketing strength.
3. What Happens When You Miss a Call?
Even elite admissions teams will miss calls during peak volume, shift changes, lunch breaks, or after-hours windows. The question is not whether misses happen—it’s whether there’s a structured recovery system in place to catch them immediately.
One layer of protection is speed-to-response automation. When a call is missed or a form is submitted, an automated text can be triggered within 60 seconds through a CRM integration. This message lets the prospective patient or loved one know that someone will be reaching out within the next five minutes and asks them to stay available. That simple touchpoint reduces the likelihood that they continue calling other providers, because they now expect a prompt follow-up.
Another highly effective safeguard is partnering with a dedicated overflow provider like Rollover Rep.
Rollover Rep is a specialized behavioral health answering and admissions support service designed specifically for treatment centers. Instead of routing missed calls to voicemail, your inbound line forwards directly to a live, trained representative when your team is unavailable.
Here is how it works operationally:
- Your primary admissions line rings internally first
- If unanswered within a set number of rings, the call automatically forwards to Rollover Rep
- Their trained representative answers live using your approved call flow and scripting
- Key qualifiers such as insurance, age, and clinical concern are gathered
- Detailed notes are documented and passed back to your team in real time
- Your admissions coordinator follows up for continuity and next steps
This dual approach—immediate automated acknowledgment plus live overflow coverage—protects answer rate, protects revenue, and most importantly protects the caller from hitting silence during a vulnerable moment.
Because Rollover Rep focuses specifically on behavioral health, they understand insurance conversations, clinical triage basics, and the urgency that often accompanies these calls. That specialization matters.
If you rely solely on voicemail and delayed callbacks, you are accepting unnecessary leakage. A structured system that combines instant communication with live backup ensures that even when your internal team is unavailable, the caller still receives a timely, professional, and compassionate first touch.
4. Do You Score Your Calls?
Before you can understand which marketing channels are working, you need a standardized scoring system applied to every single inquiry.
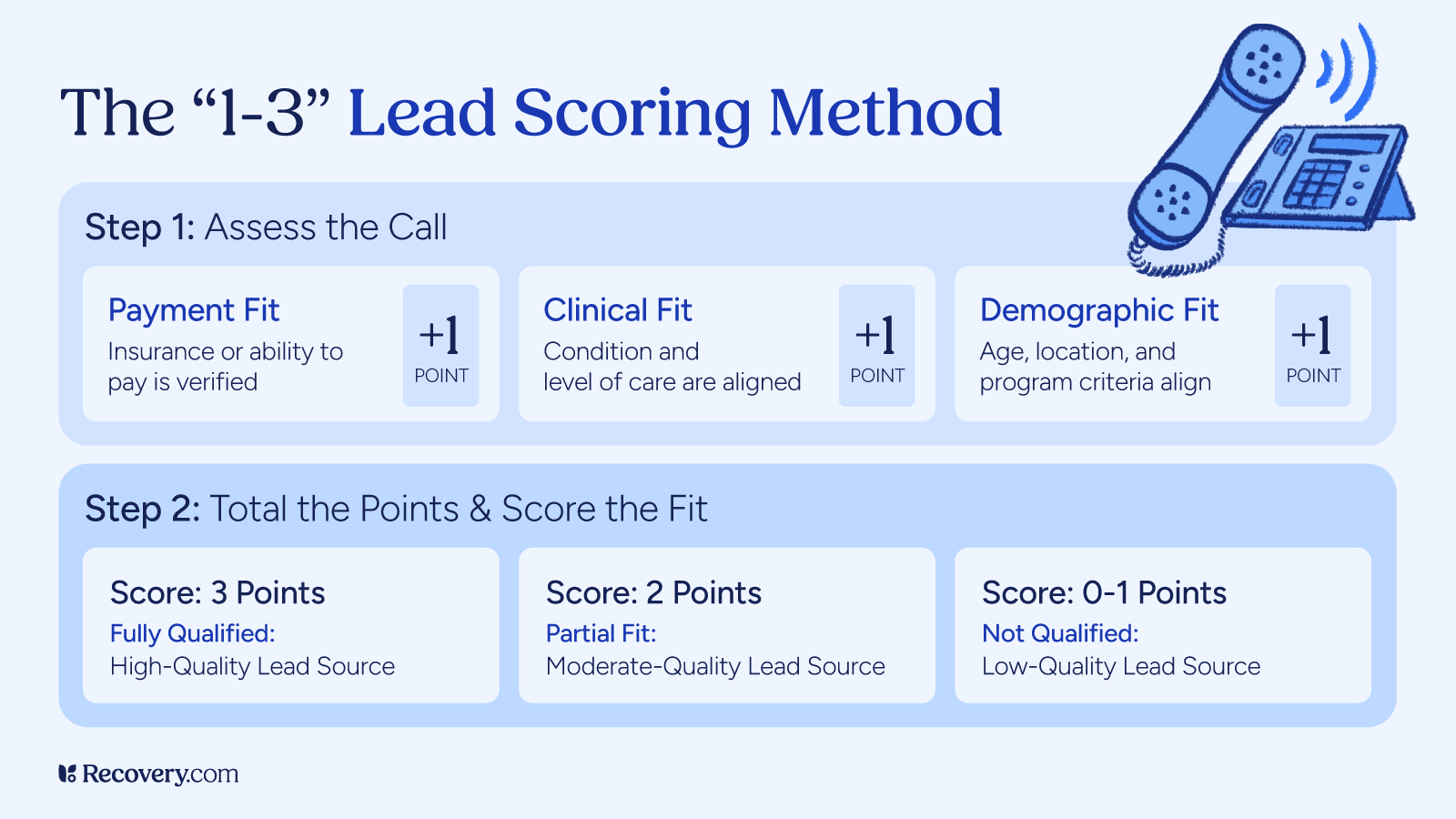
The 1 to 3 qualification model becomes essential.
Every inbound call or form submission should be scored using the same three criteria:
- Payment eligibility: They can pay for your treatment or have insurance you accept
- Clinical fit: You can treat the condition they need help with at the acuity they have it.
- Demographic fit: Age, gender, location, etc.
Score 3 means all three criteria align.
Score 2 means exactly one criterion is misaligned.
Score 1 means multiple criteria are misaligned.
If admissions teams are not consistently assigning a score and documenting referral source, you do not truly know which marketing channels are producing qualified opportunities. You have opinions. You have anecdotes. You have vibes.
But you do not have clean attribution data.
This gives you a comparative quality index across channels, not just volume.
When this is done consistently, leadership can clearly see:
- Which channels produce the highest percentage of fully qualified leads
- Which channels generate volume but low clinical or financial fit
- Where marketing dollars are driving real admissions versus noise
Without standardized scoring, budget decisions become emotional.
One coordinator might say, "We get great calls from this source."Another might say, "Those leads never admit."
Both may be partially correct. Only structured scoring resolves the debate.
A simple 1 to 3 framework, applied consistently and tied to referral source, transforms admissions from a feeling-driven function into a measurable performance engine.
It is not about labeling people.
It is about building a feedback loop that tells you where your best opportunities are actually coming from.
5. How Fast Do You Respond To Form Submissions & VOBs?
High-performing behavioral health admissions teams strive to make first contact within 5 minutes or less during business hours. Response times beyond 10 minutes begin to see measurable drops in connection rates.
If submissions come in after hours, there should be an immediate automated text response within 60 seconds, followed by a live outreach attempt first thing the next morning, ideally within 15 minutes of opening.
Speed is not about pressure. It is about meeting urgency with presence.
Form submissions often represent high intent with lower comfort calling.
How quickly does outreach happen? Are there multiple contact attempts? Are phone, text, and email all being used strategically?
Delays significantly reduce connection rates.
Forms should be treated with the same urgency as live calls.
6. Do You Have A Living “Obstacle Overcomes” Document?
Every behavioral health admissions team should maintain a living, shared document called Obstacle Overcomes.
This is not a private notebook. It is not something that lives in one coordinator’s head. It is a dynamic, visible document that the entire admissions team contributes to and reviews regularly.
Here is how it works.
When an admissions coordinator encounters an objection or obstacle on a call, they log it in the document. If they successfully navigated it and the caller moved forward, they document the language and approach that worked. If they were not successful, they document the obstacle anyway so the team can collaborate on stronger “overcomes” for the future.
Over time, patterns emerge.
Cost concerns.Time away from work or family.Fear that treatment will not work.Concerns about stigma.Worries about academic or job disruption.
Instead of reacting to these in isolation, the team builds a shared playbook.
This document should include:
- The obstacle stated in the caller’s own language
- Context about when it came up in the call
- The response used
- The outcome
- Alternative language to test in future calls
If a coordinator struggles with a particular objection, the team supports them in developing new approaches. This turns missed opportunities into training assets.
But this document is not just a reference tool. It is a training tool.
New admissions coordinators should be drilled on this document before they ever go live on the phones. During onboarding, leadership should:
- Review the most common obstacles line by line
- Role play real call scenarios using documented objections
- Practice multiple overcome approaches
- Refine tone, pacing, and confidence
- Simulate high-emotion calls before real exposure
No new team member should encounter a predictable objection for the first time on a live call.
The Obstacle Overcomes document allows teams to rehearse real-world friction in a controlled environment. It shortens ramp time, increases consistency, and builds confidence.
But this document should not stay within admissions.
It should be shared directly with marketing.
Obstacle data is one of the most powerful drivers of content strategy. If callers consistently express fear about leaving their job, marketing should create content addressing job protection and FMLA. If families worry about whether treatment works, there should be outcome data, testimonials, videos, podcasts, and articles ready to share.
Imagine a caller says they are worried about something specific, and the admissions coordinator can immediately respond with:
- A short explainer video
- A helpful graphic
- A podcast episode
- A detailed article
- Or all of the above
That level of preparedness builds trust.
It communicates that the center understands the concern deeply enough to have created resources around it.
Objection handling is not persuasion. It is clarity supported by evidence and education.
A living Obstacle Overcomes document transforms objections from friction points into feedback loops. It strengthens admissions performance, accelerates onboarding, and directly informs marketing content creation.
When admissions and marketing are aligned around real-world caller concerns, conversion improves and trust deepens.
7. Do You Role Play With Your Admissions Team?
The fastest way to improve admissions performance isn’t just more calls—it’s structured practice before the calls ever happen.
Admissions is a skill. And like any skill, it improves with repetition—but only if that repetition is intentional.
That’s where role play becomes critical.
Top-performing teams don’t wait for real calls to train. They simulate them.
They practice:
- High-emotion conversations
- Common objections
- Deep discovery
- Confident closes
And they don’t just “run through it”. They use a standardized call flow rubric to score performance.
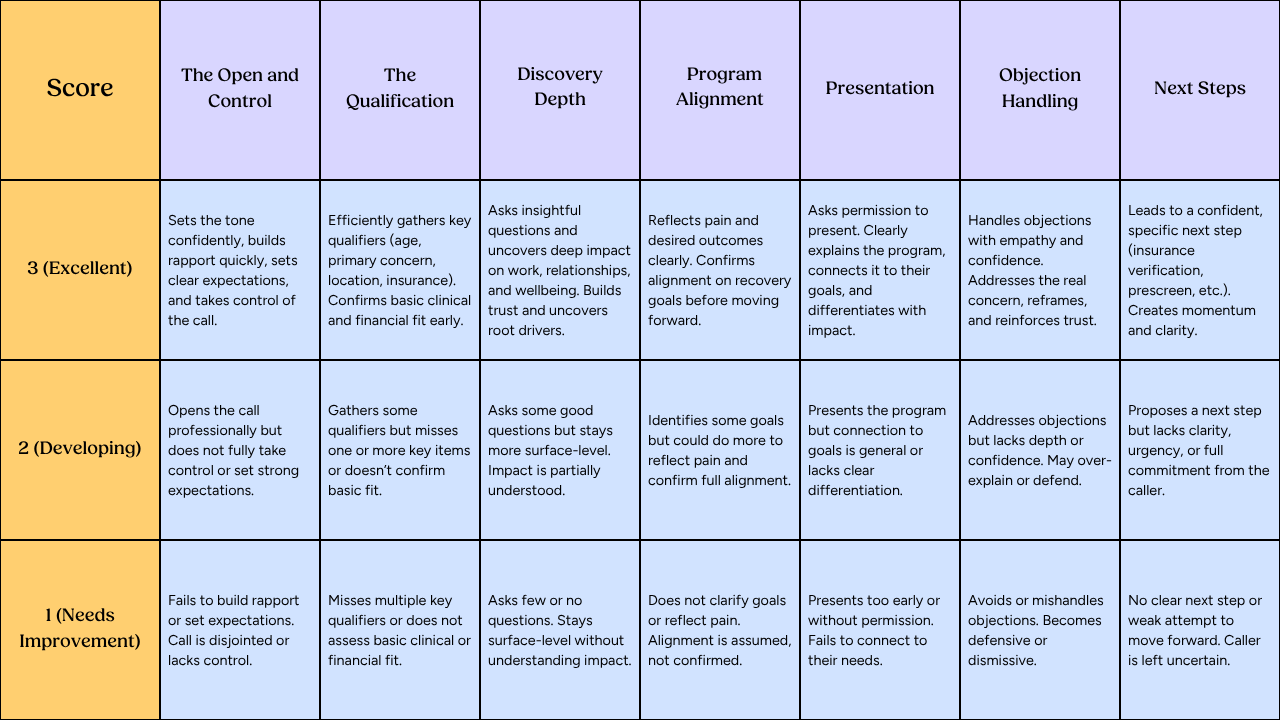
Instead of vague feedback like “that was good” or “dig deeper,” teams evaluate specific parts of the call:
- The open and control
- Qualification
- Discovery depth
- Alignment
- Program presentation
- Objection handling
- The close
Each area is scored, making it clear exactly where improvement is needed.
This same process should happen during onboarding—before anyone takes a real call.
No predictable objection or scenario should feel new when it happens live.
Where AI Fits In
AI role play tools can take this even further.
Platforms like Time Machine allow teams to:
- Simulate real conversations
- Practice difficult scenarios
- Get immediate feedback
- Repeat without risk
AI doesn’t replace coaching—it scales it.
Bottom Line
Teams that practice with structure perform with consistency.
Because when preparation goes up, variability goes down—and admissions outcomes improve.
The Bigger Question
Before increasing marketing spend, every behavioral health center should ask a harder question.
Is our admissions system structured enough to turn opportunity into measurable performance?
Do we have:
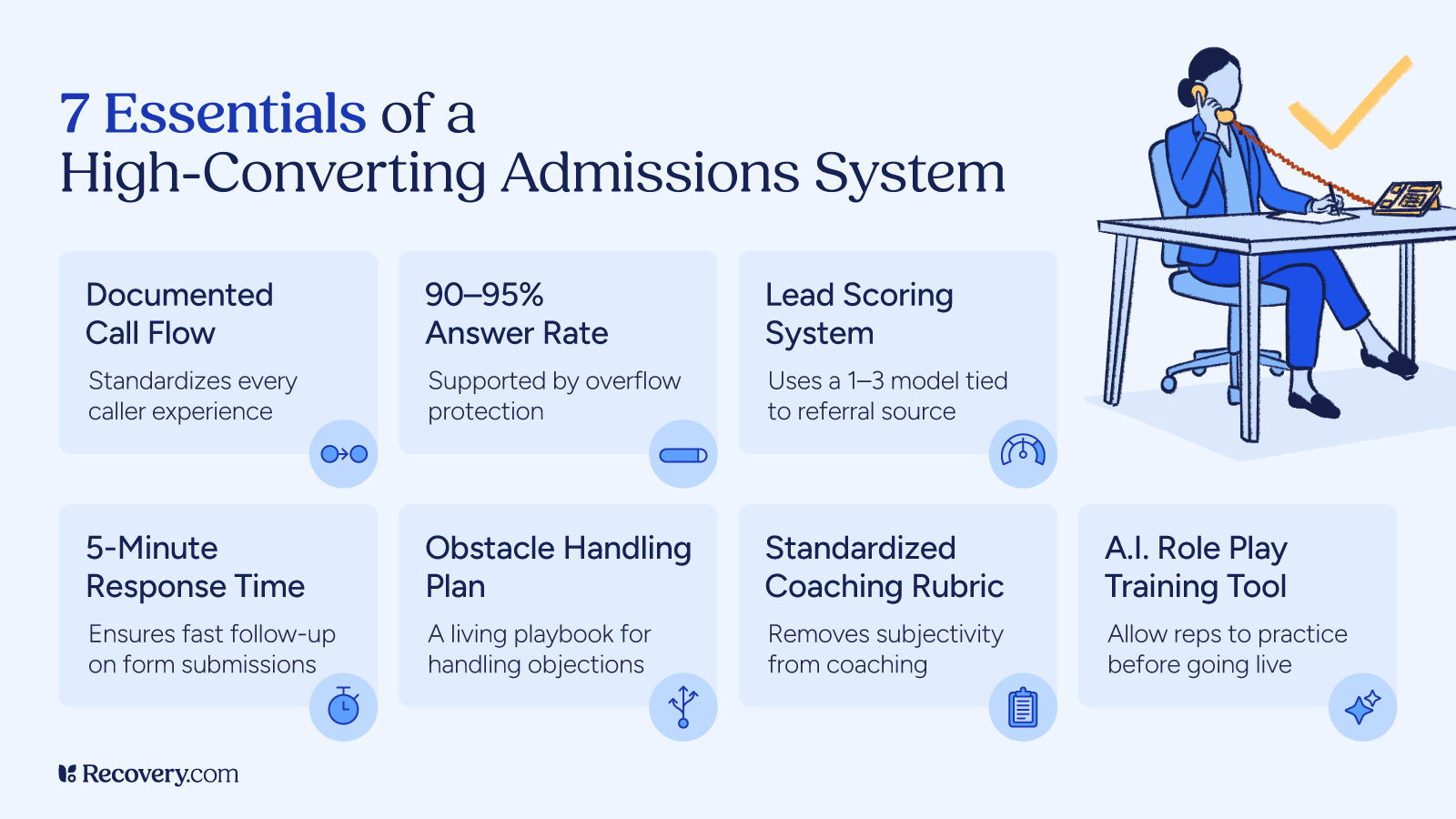
- A documented call flow that standardizes every caller’s experience?
- A 90 to 95 percent answer rate supported by overflow protection like Rollover Rep?
- A 1 to 3 scoring system tied to referral source so we know which channels are actually producing qualified leads?
- A clear five-minute response benchmark for form submissions?
- A living Obstacle Overcomes document that strengthens both admissions training and marketing content?
- A standardized rubric that removes subjectivity from coaching?
- AI role play tools that allow reps to practice before they ever go live?
If the answer is no to any of these, the issue is not traffic.
It is infrastructure.
Admissions is not just a department. It is the conversion engine of the organization.
When admissions is standardized, scored, documented, drilled, and continuously improved, marketing stops being a gamble and starts becoming a predictable growth channel.
The most important question is not how many calls are coming in.
It is whether your system is disciplined enough to turn those calls into care.
Our Promise
How Is Recovery.com Different?
We believe everyone deserves access to accurate, unbiased information about mental health and recovery. That's why we have a comprehensive set of treatment providers and don't charge for inclusion. Any center that meets our criteria can list for free. We do not and have never accepted fees for referring someone to a particular center. Providers who advertise with us must be verified by our Research Team and we clearly mark their status as advertisers.
Our goal is to help you choose the best path for your recovery. That begins with information you can trust.