Find Treatment By
Rehabs by Location






Learn
About Us
Recovery.com combines independent research with expert guidance on addiction and mental health treatment. Our mission is to help everyone find the best path to recovery through the most comprehensive, helpful network of treatment providers worldwide.
Advisory Council
Our advisory council brings together leaders in behavioral health, technology, and business. Their diverse expertise ensures our resources and product are innovative, evidence-based, and effective. They guide our mission as accomplished individuals dedicated to improving the landscape of addiction recovery and mental wellness.
Behavioral Health Admissions: 5 Call Flow Steps That Convert More Inquiries Into Placements

This call flow is grounded in Motivational Interviewing (MI) best practices. The goal is not to pressure or persuade, but to guide the caller toward their own clarity and commitment.
Admissions experts should:
- Use open-ended questions
- Practice reflective listening
- Affirm strengths and intentions
- Develop discrepancy between current reality and future goals
- Support autonomy and choice
The structure below creates direction and leadership while maintaining empathy, collaboration, and respect for the caller's decision-making process.
Phase 1: Open & Qualify
1. THE OPEN – TAKE CONTROL
Objective: Establish leadership and direction immediately.
"Thank you for calling [Center Name], this is [Name]. Who am I speaking with today?"
"And are you calling for yourself or someone else?"
Initial Qualifiers
- Age of client
- Primary concern (mental health, substance use, or both)
- Current location
- Insurance type (private, Medicaid/Medicare, self-pay)*
- Referral source (How did you hear about us?)
*If payment doesn't align, share a curated Recovery.com list of treatment options that match their insurance or budget needs
2. SET EXPECTATIONS (CONTROL + FIT)
"I want to make sure we're the right fit. We keep availability limited to protect quality, so I'll ask a few questions to see if we're the best option. And if we're not, I'll help you find the right resources. Sound okay?"
Phase 2: Discovery & Goal Setting
3. DISCOVERY – PAIN, DIG, GET REAL
Open-Ended Start
"What made you concerned enough to reach out today?"
Core Dig Questions
- How long has this been going on?
- What else have you tried?
- What was missing from those attempts?
- How is this affecting school or work?
- How is this affecting relationships?
- How is this affecting you personally?
Deepening Questions
- If nothing changes, where do you see this six months from now?
- If we fast-forward two years, what worries you most?
4. DEFINE FUTURE GOALS IN RECOVERY
Shift the focus from pain to possibility and identify the goals that hope recovery will help them achieve.
"If treatment works the way you hope it will, what does life look like six months from now?"
"What would be different day-to-day, in routines, relationships, or mindset?"
"What are you hoping recovery gives back: stability, trust, independence, peace?"
Phase 3: Align & Present
5. OVERVIEW – REFLECT BACK (YES ALIGNMENT)
The admissions expert should clearly reflect both the problem and the recovery goals back to the caller, then ask for confirmation and continue clarifying until they hear a clear "yes." This ensures alignment and demonstrates true understanding.
"So what I'm hearing is the anxiety has gotten to the point where you're missing work, your marriage is strained, and you're scared this could get worse. And what you want is stability, clarity, and to feel like yourself again. Did I get that right?"
(Wait for confirmation.)
6. TRANSITION – ASK PERMISSION TO PRESENT
"Would it be helpful if I explained how our program is designed to address exactly what you just described?"
7. THE PROGRAM – BIOPSYCHOSOCIAL MODEL
"We use what's called a biopsychosocial model. It's like a three-legged stool. If one leg is missing, recovery becomes unstable."
1. Biological Care
- Safe detox (if needed)
- Medication management
- Sleep stabilization
- Nutrition
- Medical oversight
"If someone is exhausted, malnourished, or chemically unstable, therapy won't stick."
2. Psychological Care
- Individual therapy
- CBT / DBT
- Trauma-informed care
- Coping skills development
- Emotional regulation work
"This is where we address the underlying thought patterns and behaviors driving the struggle."
3. Social Care
- Group therapy
- Family therapy
- Rebuilding support systems
- Environmental restructuring
"Isolation and toxic environments keep people stuck. We repair and rebuild support systems."
Personalize
"Based on what you shared about ____, this model directly addresses that."
Phase 4: Differentiate & Close
8. DIFFERENTIATION (WHY YOUR CENTER)
Clearly articulate distinguishing features:
- Age-specific programming
- Small group sizes
- Individualized treatment planning
- Evidence-based therapies
- Family integration
- Academic or vocational support (if applicable)
Tie each feature back to their stated pain points.
9. INSURANCE & NEXT STEPS
At this stage, the admissions expert should confidently move into collecting specific insurance details or scheduling the next step.
Insurance Collection
"To check your benefits and coverage, I'll need a few details from your insurance card."
- Insurance provider name
- Member ID number
- Group number (if applicable)
- Policy holder name and date of birth
- Relationship to policy holder
Set expectations clearly:
"We'll verify your benefits and call you back with a clear understanding of coverage and any potential out-of-pocket costs."
Scheduling the Next Step
If appropriate, move directly to scheduling:
"The next step is a confidential clinical pre-screen. It takes about 20 minutes and helps us determine the appropriate level of care. I have availability today at ___ or tomorrow at ___. Which works better for you?"
Always assume forward progress and guide them into action.
Phase 5: Handle Objections & Reinforce
10. OBJECTION NAVIGATION
"Usually when someone hesitates, it's one of three things: cost, time away from responsibilities, or uncertainty about whether it will work. Which one feels biggest for you?"
Cost
- Verify insurance benefits
- Explore payment plans
- Discuss financial options if available
Time / Family Responsibilities
"If nothing changes, how much more time might be lost?"
Fear It Won't Work
"What didn't work about the last program?"
Differentiate clearly and calmly.
11. REINFORCE THE DECISION
"You called today for a reason."
"The version of you six months from now will either be glad you acted, or wish you had."
Maintain calm, grounded tone.
12. CLOSE – NEXT STEP (NOT HARD SELL)
Always close on the next clinical step:
- Insurance verification
- Clinical pre-screen
- Assessment scheduling
"The next best step is a confidential clinical pre-screen. It takes about 20 minutes. I have openings today at 3:00 or tomorrow morning. Which works better?"
Assume forward movement.
CORE PRINCIPLES
- Take control early
- Dig deep into pain and impact
- Clarify goals and motivation
- Reflect before presenting
- Sell the experience through biopsychosocial care
- Reinforce decision calmly
- Close on the next step, not on pressure
Call Scoring Rubric
Here is an example call flow scoring rubric for behavioral health treatment centers:
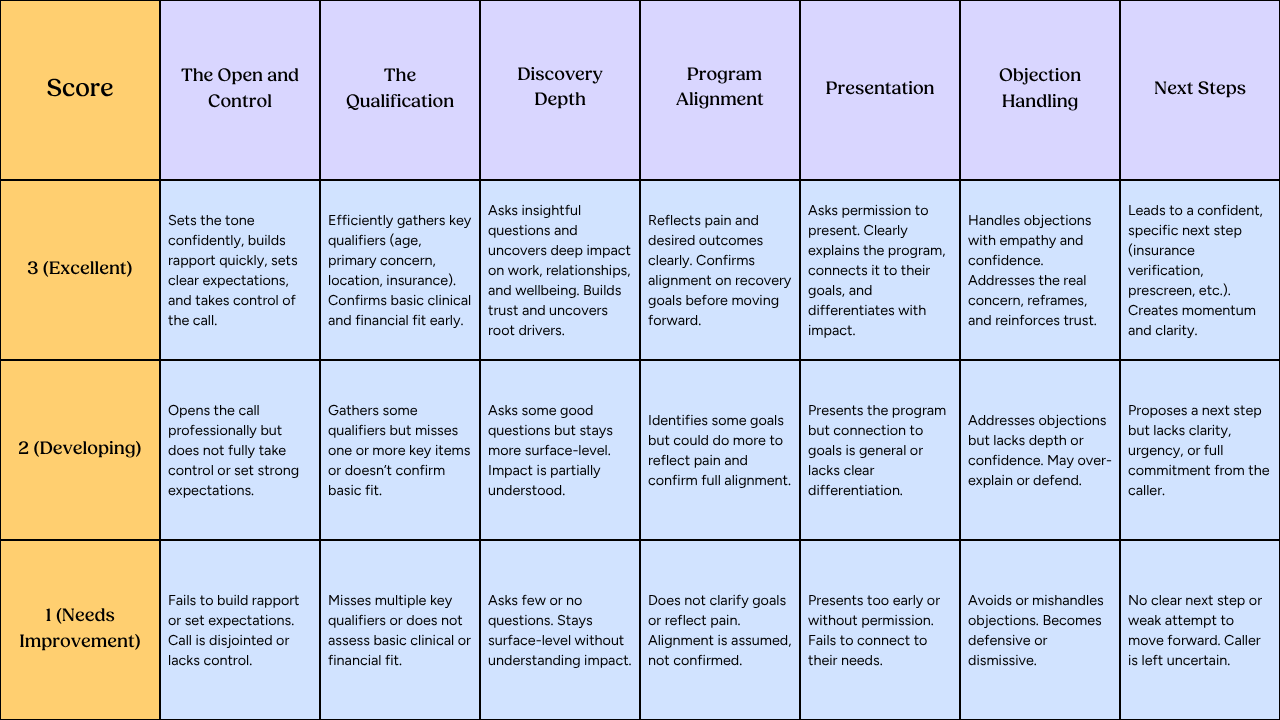
Scoring Structure
Each call is scored across 7 categories:
- Open and Control
- Qualification
- Discovery
- Depth Alignment
- Presentation
- Objection Handling
- Next Steps
Each category is scored from 1 to 3.
- Maximum total score: 21
- Minimum total score: 7
You can evaluate performance using either:
- Total Score (out of 21)
- Average Score (Total ÷ 7, on a 1–3 scale)
Performance Ranges
Excellent (Top Performer)
- Total Score: 18–21
- Average Score: 2.6 – 3.0
What this means:
- The rep is consistently strong across the entire call
- Minor gaps may exist, but they don’t impact outcomes
- Calls are structured, intentional, and conversion-focused
These reps:
- Build trust quickly
- Uncover real needs
- Confidently guide callers to clear next steps
Developing (Mid-Level Performance)
- Total Score: 13–17
- Average Score: 1.9 – 2.5
What this means:
- The rep shows competence but lacks consistency
- Some parts of the call are effective, others are surface-level or missed
- Opportunities to convert are being left on the table
These reps:
- Need targeted coaching in specific sections
- Often understand the process but don’t fully execute it
Needs Improvement (At Risk)
- Total Score: 7–12
- Average Score: 1.0 – 1.8
What this means:
- The call lacks structure, depth, or control
- Key stages are skipped or mishandled
- High likelihood of lost or poorly qualified admissions
These reps:
- Require foundational coaching
- May need retraining on call flow and objectives
How to Use This Practically
- Quick evaluation: Use total score for fast benchmarking
- Coaching: Use category-level scores to diagnose issues
- Tracking progress: Monitor average score over time
- Team benchmarks: Set minimum standards (e.g., 2.5 average)
Simple framing
- 18–21 (2.6–3.0 avg) → Strong, consistent, high-converting
- 13–17 (1.9–2.5 avg) → Capable but inconsistent
- 7–12 (1.0–1.8 avg) → Needs immediate improvement
Our Promise
How Is Recovery.com Different?
We believe everyone deserves access to accurate, unbiased information about mental health and recovery. That's why we have a comprehensive set of treatment providers and don't charge for inclusion. Any center that meets our criteria can list for free. We do not and have never accepted fees for referring someone to a particular center. Providers who advertise with us must be verified by our Research Team and we clearly mark their status as advertisers.
Our goal is to help you choose the best path for your recovery. That begins with information you can trust.