Find Treatment By
Rehabs by Location






Find Treatment By
Learn
About Us
Recovery.com combines independent research with expert guidance on addiction and mental health treatment. Our mission is to help everyone find the best path to recovery through the most comprehensive, helpful network of treatment providers worldwide.
Advisory Council
Our advisory council brings together leaders in behavioral health, technology, and business. Their diverse expertise ensures our resources and product are innovative, evidence-based, and effective. They guide our mission as accomplished individuals dedicated to improving the landscape of addiction recovery and mental wellness.
The History of Treatment Center Marketing: 7 Top Changes & What Is Next
Clint Mally is the Vice President of Content at Recovery.com, where he leads creative strategy rooted in one guiding belief: communication is a form of care. Drawing on his background in education, storytelling, and behavioral health marketing, he helps make recovery information accessible, empathetic, and empowering.
Clint Mally is the Vice President of Content at Recovery.com, where he leads creative strategy rooted in one guiding belief: communication is a form of care. Drawing on his background in education, storytelling, and behavioral health marketing, he helps make recovery information accessible, empathetic, and empowering.
If you work in behavioral health, you have probably felt it, what used to work for treatment center marketing does not work the same way anymore. Ten years ago, you could spend aggressively on ads, get in front of people in crisis, and keep the phones ringing. Today, that same approach can drain your budget, damage your reputation, and still leave beds empty.
In this episode of Recovery Reach, I sit down with Nick Jaworski, CEO of Circle Social Inc, an agency focused specifically on treatment centers. Nick has been in the industry for over a decade, and he walks through what the last ten years of addiction treatment marketing looked like, why it changed, and what treatment centers should do now to build trust, grow sustainably, and prepare for AI driven search.
Here are the biggest takeaways, in plain English, with practical implications for treatment center owners, marketing teams, and operators.
1. From Visibility to Credibility
Nick describes the early days of behavioral health marketing as an immature market, with tons of demand and not enough supply. During the peak of the opioid crisis, the urgency was intense. Parents were terrified, people were calling in crisis, and many families felt like they needed a bed immediately.
That urgency changed the entire marketing dynamic.
Back then, you did not need elite branding. You did not need sophisticated content. You did not even need a well run program to convert a large share of incoming leads. You mostly needed to show up first when someone searched “rehab near me” or clicked an ad in a moment of panic.
Nick’s point is not that outcomes did not matter, it is that the market conditions did not reward quality the same way they do now. When the demand wave is massive, mediocre marketing and sloppy operations can still look successful.
Today, that cushion is gone.
If you are still operating with the old mindset, “we just need more leads,” you will probably miss the real issue. The problem is rarely just volume anymore, it is trust, differentiation, and delivery.
2. The Affordable Care Act & The Ad Race
A key inflection point Nick highlights is the Affordable Care Act and parity requirements, meaning mental health and addiction treatment had to be covered more like other medical care. That shift increased access and brought insurance reimbursement into the center of the business model.
But it also created a perfect storm of incentives.
Nick explains that reimbursement rates, especially out of network, were extremely high in that era. Programs could be reimbursed tens of thousands of dollars per patient, sometimes far more across a longer stay or repeat admissions. When margins are huge, teams often stop paying attention to efficiency.
Nick shares a striking example, large providers running Google Ads campaigns with cost per acquisitions above $12,000, sometimes far higher, and not even realizing it because the money still worked.
This is one of those uncomfortable truths. When revenue is flowing, businesses rarely feel pressure to tighten systems, align teams, or build long term strategy. They keep doing what “works,” until it stops.
And in treatment center marketing, the day it stopped came fast.
3. LegitScript & Platform Crackdowns
Nick points to LegitScript and Google’s clampdowns as a major turning point. The industry had become known for shady marketing practices, patient brokering, stolen phone numbers, copycat ads, and misleading branding designed to look like reputable centers.
The core issue was trust. Families assumed they were interacting with something like traditional healthcare, but the reality did not always match the promise. Nick and I talk about the human cost here, people were harmed, families were misled, and in some cases people died.
So platforms and regulators stepped in.
The new reality is that pay per click advertising in behavioral health is not just about budget anymore, it is also about compliance, verification, and proving legitimacy. It can feel annoying for ethical providers to jump through hoops, but it also blocks some of the worst actors from easily scaling.
In other words, the floor rose.
And once the floor rises, basic competence is no longer a competitive advantage.
4. Trust became the real product
One of Nick’s most memorable explanations is his restaurant analogy.
If a restaurant markets “best steak in town” and delivers rubbery steak and slow service, marketing does not save them, it accelerates their downfall. The bigger the promise, the faster the negative reviews, bad word of mouth, and reputation damage.
Treatment centers are now in that same reality.
Nick says there must be alignment between the marketing promise and what the program actually delivers. That sounds obvious, but in practice it is where many treatment center marketing strategies fall apart.
Why?
Because treatment center organizations often operate in silos.
Marketing says one thing. Business development says another. Clinicians do something else. Admissions answers calls using a totally different script, tone, and set of assumptions.
Nick says when Circle Social goes into a program, they frequently find that the biggest growth limiter is not “ads,” it is internal misalignment. The program is not translating its strengths into a consistent story across the website, intake calls, community relationships, and real client experience.
And in a localized, review driven world, inconsistencies show up quickly.
5.The Rise Of Local Marketing
A major shift Nick calls out is localization. Search behavior, payer insights, and platform algorithms all push toward local treatment.
Nick says payers can see in their data that members who seek care closer to home often have better outcomes, fewer ER returns, less return to use, and fewer returns to treatment. That reality reinforces localization trends in referrals and search.
I frame it in a relatable way, in a small town, you behave differently because relationships matter. You will see people again. Your reputation follows you.
That is exactly what is happening with treatment center marketing now.
Even if your program can take people from anywhere, the most sustainable strategy is usually to earn trust locally, with clinicians, hospitals, therapists, alumni networks, and community partners.
Because the truth is, local trust compounds.
And trust compounds faster than ad spend.
6. The New Marketing Mix
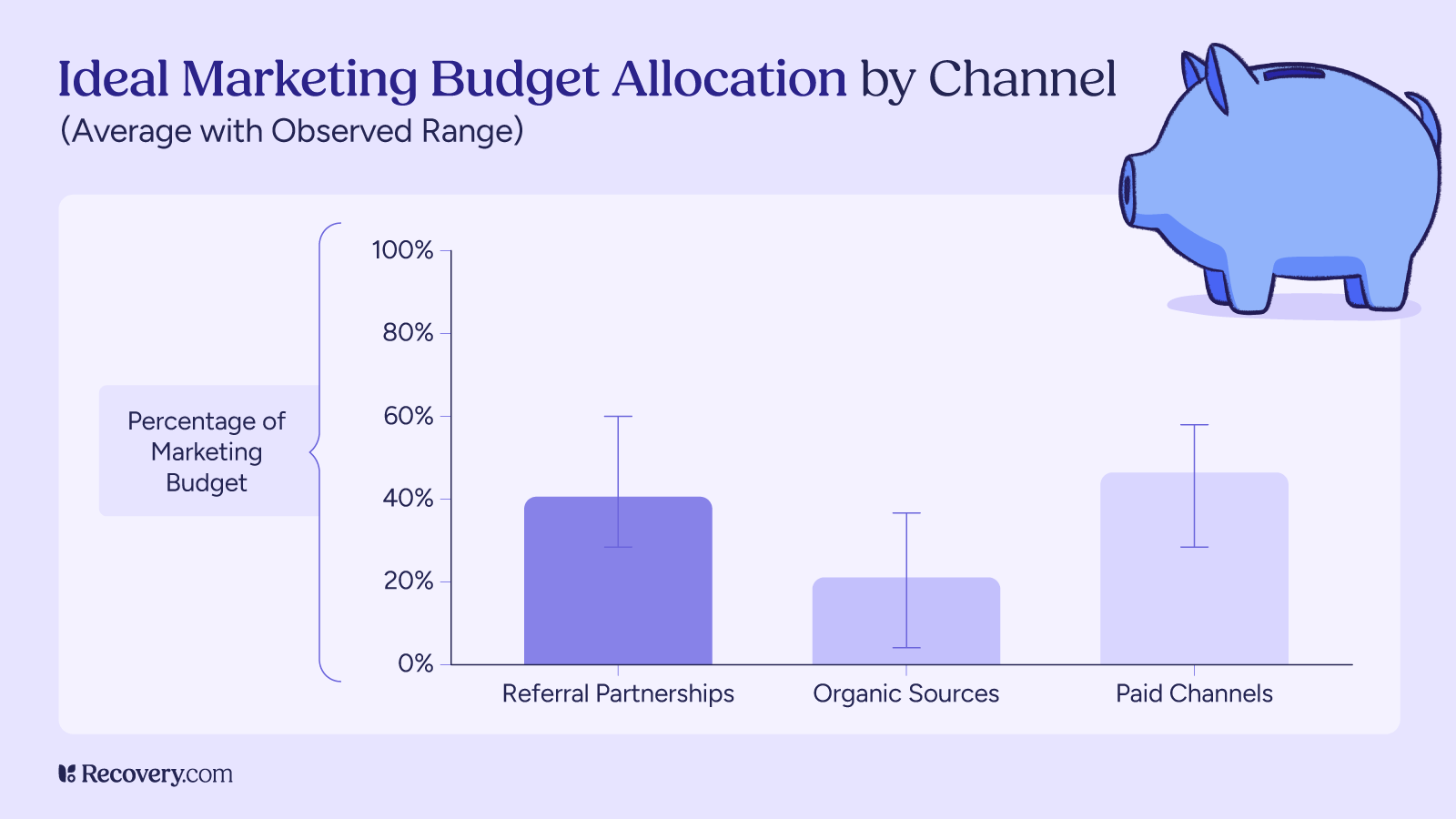
Nick shares a baseline admissions model his team has found successful across many providers. He frames it as a general benchmark, not a rigid rule, because location, level of care, and payer mix all matter.
Still, the structure is useful:
- 50% from business development and community referrals
- 20% from alumni, including referrals and readmissions
- 30% from digital, including SEO, AI optimization, and paid media
This is important because it flips how many treatment centers actually behave.
Nick and I also note that many centers spend the most on PPC, while investing the least in business development and organic growth. That creates a fragile system where a single platform change, compliance issue, or cost spike can collapse your census.
Nick’s model is basically a stability strategy.
Community referrals create resilience. Alumni creates momentum. Organic and diversified digital creates efficiency over time. PPC becomes one ingredient, not the whole meal.
If you want a sustainable treatment center marketing strategy, this is the kind of mix you are aiming for.
We actually did a whole article on marketing mix which is worth the read.
7. The Rise of AI & Third Party Trust
When the conversation turns to AI, Nick makes a clear point, AI driven discovery is coming fast, and treatment centers should invest now even if the measurable admissions volume is still small.
The reason is simple. AI optimization is not a switch you flip. It is a compounding investment.
Nick also explains something that many marketers miss, AI search often relies heavily on third party sources rather than just your website. One example he points to is Recovery.com, which AI systems already treat as a trusted, authoritative source when answering behavioral health and treatment related queries. Your site is “marketing collateral.” AI systems look for verification in places that feel more objective, including well known third party platforms like Recovery.com, reputable directories, and established media outlets.
This is where I share a few practical tactics you can apply right away.
AI marketing looks more like old school reputation building:
- Get mentioned by credible local sources
- Sponsor events that lead to community coverage
- Show up in trusted directories and third party platforms
- Keep facts consistent across the internet, because AI gets “confused” by discrepancies
- Refresh content frequently, especially local content, so you stay current
Nick notes that this is exactly why AI optimization can be hard, you cannot fully control third party narratives the way you can control your website.
But you can influence them through consistent community presence, clear positioning, and strong relationships.
That is also why local wins again.
A national brand can publish broad content, but a local provider can become the most trusted answer for a specific city, county, and referral ecosystem. That is where AI driven search is likely to produce outsized benefits for organizations willing to invest early.
The biggest lesson
Treatment center marketing used to be about urgency and visibility. Now it is about alignment, reputation, and trust that holds up under scrutiny, online, locally, and across AI driven discovery.
If your growth strategy is still built on “turn ads on and fill beds,” you will likely keep running into higher costs and lower conversions. The centers that win now are the ones that build trust in the community, deliver on what they promise, and invest in marketing channels that compound over time.
If you want the full context and nuance, listen to the full episode with Nick Jaworski on Recovery Reach. And if you found these insights helpful, share the post with someone on your team, especially anyone working in admissions, business development, or leadership, because marketing only works when the whole organization is telling the same story.
Our Promise
How Is Recovery.com Different?
We believe everyone deserves access to accurate, unbiased information about mental health and recovery. That's why we have a comprehensive set of treatment providers and don't charge for inclusion. Any center that meets our criteria can list for free. We do not and have never accepted fees for referring someone to a particular center. Providers who advertise with us must be verified by our Research Team and we clearly mark their status as advertisers.
Our goal is to help you choose the best path for your recovery. That begins with information you can trust.